Protein
Proteinuria is defined as the excretion of various proteins in urine.
The composition of urine protein is a mixture of high and low molecular weight proteins (see table below). Proteins are selected by the glomerular filtration as a function of their molecular weight. The threshold is about 60 kD. Proteins of low molecular weight (<40 kD) can pass through the glomerular membrane. The passage of proteins (i.e. albumin) is not only based on their molecular weight but also on their electrical charge . 99% of low molecular weight proteins are reabsorbed and catabolized in the proximal tubule cells.

Test strip, from left to right: comparison colored scale, then a negative result, then a positive result, corresponding to a protenuria of about 100 mg/dl.
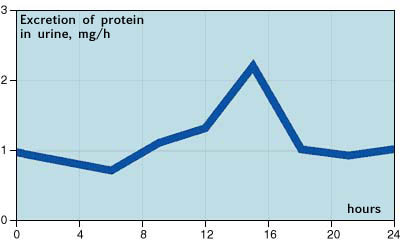
Proteinuria in healthy adults is between 50-150 mg/dl, which corresponds to the physiological concentration of protein in urine of 0.1 g/L. The excretion of protein varies during the day with a maximum in the afternoon and a minimum in the early morning (see illustration below).
| Protein | Relative molecular mass (kD) | Reference values in serum (mg/L) | Reference values in urine (mg/L) |
|---|---|---|---|
| α2-acroglobulin | 250 | M 1200-2700 F 1400-3200 |
< 10 < 10 |
| Immunglobulin G | 150 | 8000-17000 | < 10 |
| Transferrin | 79.5 | 2300-4300 | < 2.5 |
| Albumin | 67 | 37000-53000 | < 20 |
| α1-Antitrypsin | 54 | 1400-3200 | < 3.5 |
| α1-acid glycoprotein | 41 | 400-1300 | < 10 |
| α1-microglobulin | 30-33 | 25-100 | < 12 |
| Retinol-binding protein | 21 | 30-60 | < 0.5 |
| Lysozym | 14 | < 6 | < 0.3 |
| Cystatin C | 13.3 | 0.63 - 1.33 |
|
| β2-microglobulin | 13 | 1-3 | < 0.3 |
Clinical relevance
An increased and persistent proteinuria is usually due to kidney disease, while a transient increase in proteinuria may be physiological or pathological. Proteinuria provides essential evidence in the diagnosis of kidney disease in combination with microscopic examination of the sediment.
Pre-renal proteinuria
An increase in the blood concentration of low molecular weight protein leads to an increase in their filtration. The tubular maximal reabsorption capacity is exceeded, which leads to increased excretion into the urine. This is the explanation of the phenomenon known of orthostatic proteinuria (i.e. increased during the transition from supine to upright position) or of proteinuria observed after physical exercise. These are transient proteinurias and are observed most often in young adults.
Pre-renal proteinuria may occur in cases of fever, myocardial infarction, nervous system damage (i.e. stroke), emotional stress, intra-vascular hemolysis (hemoglobinuria), musculoskeletal injuries (myoglobinuria ) and myeloma (Bence-Jones proteinuria).
Renal proteinuria
Most renal proteinurias are persistent and originate in the glomerulus. The concentration in urine exceeds 0.25 g/L. It is often a marker of glomerulonephritis, in association with microhematuria. The increase in the concentration of low molecular weight proteins in blood cause an increase in their filtration. The ability of tubular reabsorption is exceeded which leads to increased excretion. Excretion of 3g /L and indicates a nephrotic syndrome.
It is seen in cases of decreased kidney function such as diabetes, lupus erythematosus or the taking of nephrotoxic drugs (i.e. aminoglycosides, cytostatics).
In the absence of proteinuria, another explanation for the decline in renal function must be looked for.
Post-renal proteinuria
Post-renal proteinuria occurs with inflammatory diseases such as cystitis, prostatitis and urinary tract bleeding.
Sensitivity, detection limit: 0.3g/L
Specificity
The test strip is particularly sensitive to albumin. Albumin has a molecular weight of approximately 66 kD, and is excreted in cases of nephropathy. The reaction on the comparison color scale corresponds to the concentration of albumin in the urine. The strip is less effective for detecting other proteins (i.e. immunoglobulins, Bence-Jones protein) so the test strip is not appropriate for the screening of multiple myeloma.
| Albuminuria - Adults | ||||
|---|---|---|---|---|
| mg/L | mg/24h | mg/g Creatinine | g/mol Creatinine | |
| Normal | < 20 | < 30 | < 20 | < 2.26 |
| Microalbuminuria | 20-200 | 30-300 | 20-200 | 2.26-33.9 |
| Albuminuria | > 200 | > 300 | > 200 | > 33.9 |
| Proteinuria | > 300 | > 450 | ||
| Albuminurie - Children (3-5 Jahre) | ||||
| Normal | < 20 | < 30 | < 3.39 | |